Welcome to a discussion about the upcoming 5th Revolution in the US, which I’ve titled the “Revenge Revolution.” For more about the Revenge Revolution and the author, click “About the Author” tab. Periodically I write a “sense check” to assess whether a revolution in the US is possible or whether the entire exercise is based on a statistical aberration — i.e., a roughly 50-year cycle between major upheavals in the US.
The previous “sense check” was ENTRY #500. Much has happened since Entry #500 to reinforce my belief we are currently embroiled in US Revolution 5, which I’ve labeled the “Revenge Revolution.”
BEGIN ENTRY #516: The gap between entries #515 and #516 was intentional, but longer than expected. A combination of waiting for the election results and another project that has essentially become full-time – and its pro bono, but a good cause.
Recent blog entries have focused on the value of education in improving economic well-being of different groups. The entries suggested the black community would do well to follow the lead of most every other ethnic group by emphasizing education for children.
After the 2024 presidential election, I’m convinced more than ever that the proper primary and secondary education is a key to economic well-being for all Americans. I’m also convinced that the education curriculum needs to revert to what was once a standard.
Based on the logic of how a large percentage of the population decided which presidential candidate to support in 2024, it is clear that America lacks a basic knowledge of history, civics, the law and other social sciences.
An unintended consequence of the effort to increase education in STEM courses – science, technology, engineering, mathematics – has been to eliminate subjects that help people learn how to think about societal issues.
Some anecdotal evidence from the election seems to point out how many people cannot connect two dots, let alone three dots. Examples:
Why did a surprisingly large percentage of blacks vote for Trump? An oft-cited response was “what have the Democrats done for me lately?”
Dot #1 – Trump does not like, nor has he supported blacks. If you have any doubts, check the list of “shithole” countries cited by Trump. Also check how Trump has repeatedly sided with and endorsed all-white ultranationalist groups.
Dot #2 – all of Trump’s proclaimed economic policies favor the wealthy. As a black, are you ready to experience major cuts in an array of social programs? And, are you ready to continue to support rulings from Trump-appointed judges to suppress voting?
Blacks were not alone in their strange voting logic. A large percentage of white seniors favored Trump.
For white seniors, do you think Trump will protect Social Security and Medicare? His cabinet nominees should not be a surprise to anyone who reads and just doesn’t get all their news from Fox.
OK, so older whites, particularly men, don’t like black women. But do you dislike a black woman so much that you’ll vote for a guy whose actions could potentially have a material negative impact on your economic well-being? The answer is “yes.”
The rationale cited by blacks, particularly men, and white seniors for voting for Trump defies logic 101. I believe it defies logic because too many people have no, or at best, have a very limited understanding of economics, history, civics, literature and other topics that enable one to think through a problem.
As a country, if we want to protect democracy and continue to increase economically, then we need to update the education curriculum to include the social sciences. People might claim that more emphasis on social sciences is elitist and even socialist.
If you’re in that camp, then I suggest you revisit the education curriculum in the era that Trump claims as America being “great.” As you review the courses, you’ll be surprised at what constituted a basic education for all students.
You might also be surprised at the array of “skilled trades” that were taught in high school. These students often were able to work in the trades immediately after high school. A high percentage of those jobs when “America was great” were in the…yikes!…union.
As we return to a basic core curriculum, we can adjust the content of the STEM subjects to address current challenges facing American industry. Doing so will help all future generations. All for now. END ENTRY #516
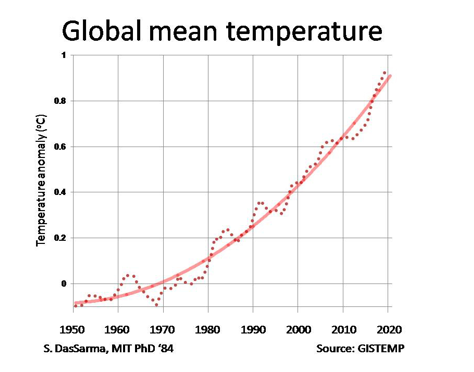
Other Topics. Interested in more info about climate change, what’s required to electrify a fleet of cars/trucks, and an array of other topics, visit another page of this website, https://usrevolution5.com/jrd-thought-comments/